
Shoulder dystocia is a rare but serious obstetric emergency that occurs during vaginal delivery. The baby’s shoulders become stuck after the head delivers, which prevents the rest of the body from emerging normally. While uncommon, shoulder dystocia requires immediate recognition and a coordinated response to reduce the risk of injury to both the baby and the mother.
What makes shoulder dystocia particularly challenging is that it is largely unpredictable. Many cases occur without warning and in pregnancies without known risk factors. As a result, labor and delivery teams train to recognize and manage it quickly. Follow along using the image below.
What Is Shoulder Dystocia?
Shoulder dystocia occurs when one or both fetal shoulders become stuck in the pelvis after the head delivers. Most often, the anterior shoulder becomes stuck behind the maternal pubic bone. Less commonly, the posterior shoulder becomes stuck against the sacrum.
This condition occurs in approximately 0.2 to 3 percent of vaginal deliveries. Clinicians do not formally diagnose shoulder dystocia until gentle downward traction on the fetal head fails to deliver the shoulders. Once clinicians identify shoulder dystocia, they must act immediately to reduce the risk of complications such as oxygen deprivation, arm nerve injury, excessive bleeding, or severe perineal trauma.
Early Recognition and Immediate Actions
Shoulder dystocia is often recognized within seconds after the baby’s head is delivered. One of the most well known signs is the turtle sign. This occurs when the baby’s head emerges and then retracts slightly back toward the perineum, resembling a turtle pulling into its shell.
When shoulder dystocia is suspected, several critical steps happen immediately:
- Shoulder dystocia is clearly announced so the entire team is aware.
- Additional help is called to the room.
- Maternal pushing is stopped.
- Excessive traction on the baby’s head is avoided.
- A mediolateral episiotomy may be considered to allow room for internal maneuvers, though it does not resolve the obstruction itself.
Early recognition and calm, structured management are essential for a safe outcome.
First Line Shoulder Dystocia Maneuvers
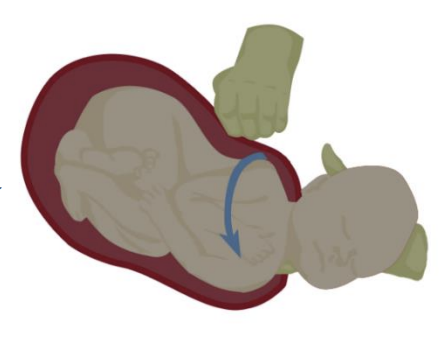
McRoberts Maneuver
The McRoberts maneuver is the first and least invasive maneuver used to manage shoulder dystocia. The mother’s hips are sharply flexed so that her thighs are brought tightly toward her abdomen. This movement flattens the lower spine and rotates the pelvis, increasing the space available for the baby’s shoulders to pass through.
This maneuver alone resolves many cases of shoulder dystocia and serves as the foundation of management.
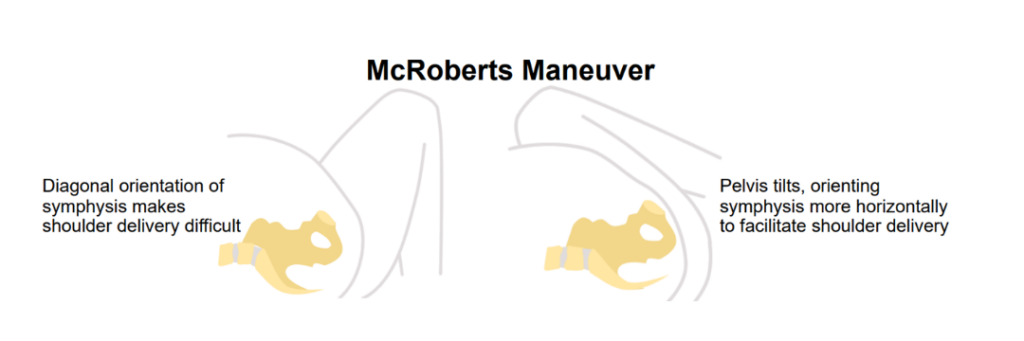
Suprapubic Pressure
Clinicians usually perform suprapubic pressure at the same time as the McRoberts maneuver. They apply firm pressure just above the pubic bone, directing it downward and slightly sideways toward the baby’s chest. The goal is to rotate and narrow the shoulders so they can move into a wider part of the pelvis.
It is important to note that suprapubic pressure is different from fundal pressure. Fundal pressure is never appropriate in shoulder dystocia and can worsen the impaction.
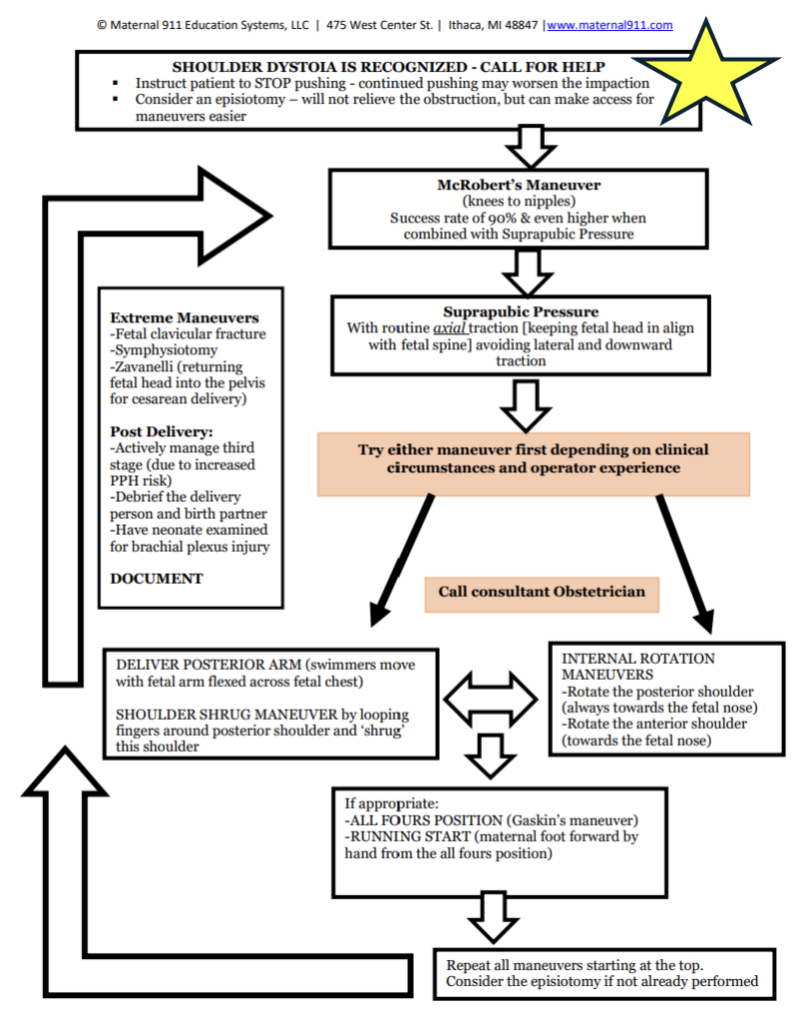
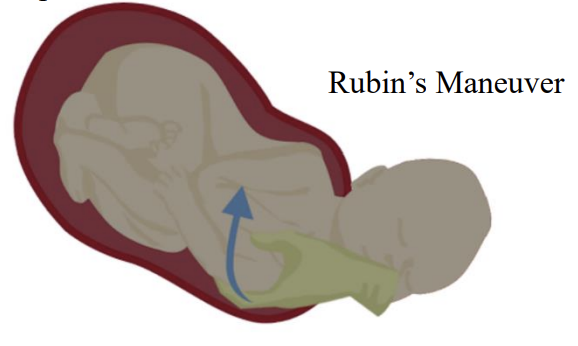
Internal Rotation Maneuvers
If external maneuvers do not resolve the dystocia, internal rotation maneuvers may be used. These involve the clinician placing a hand inside the vagina to gently rotate the baby’s shoulders into a more favorable position.
The Rubin maneuver focuses on rotating the posterior shoulder toward the baby’s face to reduce shoulder width. The Woods screw maneuver builds on this concept by progressively rotating the shoulders in a corkscrew motion. These maneuvers can be highly effective and may reduce the risk of certain fetal injuries when performed correctly.

The Woods screw maneuver builds on this concept by progressively rotating the shoulders in a corkscrew motion. These maneuvers can be highly effective and may reduce the risk of certain fetal injuries when performed correctly.
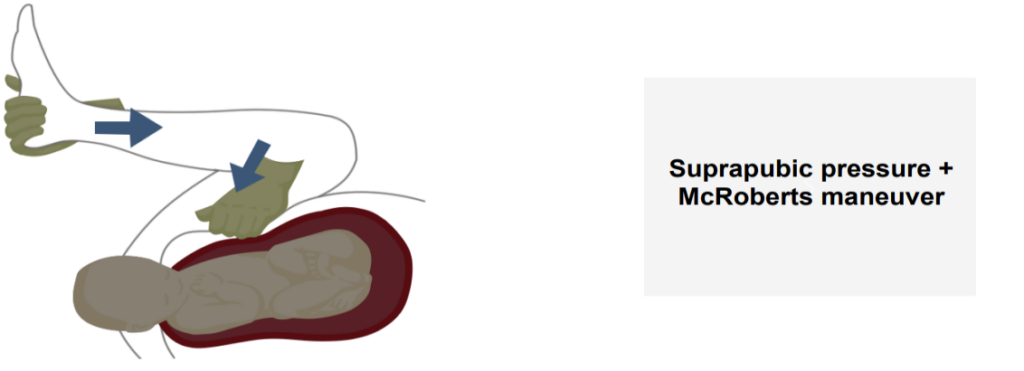
Delivery of the Posterior Arm
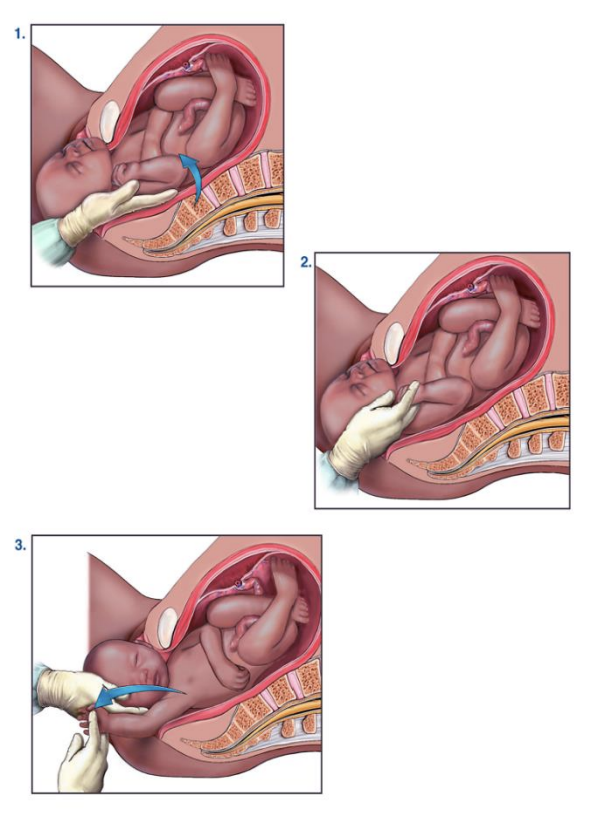
Delivery of the posterior arm is one of the most effective maneuvers for resolving shoulder dystocia. The clinician reaches the baby’s posterior arm, bends it at the elbow, and gently sweeps it across the chest and out of the birth canal. This reduces the width of the shoulders and often allows the rest of the body to deliver smoothly.
Clinicians sometimes refer to this maneuver as the swimmer’s move, and it has one of the highest success rates among shoulder dystocia techniques. In more difficult cases, clinicians may use additional tools, such as a soft catheter, to assist with traction on the posterior shoulder.
Maternal Position Changes
All Fours Position
Changing the mother’s position can also help resolve shoulder dystocia. Repositioning onto hands and knees, also known as the all fours or Gaskin maneuver, can increase pelvic dimensions and allow gravity to assist with delivery.

In some cases, this position alone resolves the dystocia. In others, it improves access for additional maneuvers. This technique requires the mother to move, which epidural anesthesia or exhaustion may limit.
What Should Never Be Done
Certain actions are never appropriate during shoulder dystocia:
- Fundal pressure should never be applied.
- Excessive pulling on the baby’s head should be avoided.
- Maneuvers should not be repeated without reassessment or a clear reason.
Avoiding these actions helps reduce the risk of injury.
Extreme Maneuvers
In very rare and severe cases where standard maneuvers fail, extreme measures may be considered. These include intentional fracture of the baby’s clavicle, surgical widening of the pelvis, or replacement of the baby’s head followed by emergency cesarean delivery.
These maneuvers carry significant risks and are reserved only for life threatening situations when all other options have failed.
Post Delivery Care
After delivery, both the mother and baby require careful assessment. Clinicians examine the baby for signs of nerve injury or fractures, many of which resolve on their own over time. They monitor the mother closely for bleeding, perineal injury, and other complications.
Debriefing the care team and the family is also an important part of post delivery care.
Documentation After Shoulder Dystocia
Thorough documentation is critical after a shoulder dystocia. This includes:
- The time from head delivery to full delivery
- The sequence and timing of maneuvers used
- All personnel present during the event
- Maternal and neonatal outcomes
Clear documentation supports quality improvement and provides important medical and legal clarity.
Shoulder dystocia is a stressful event, but prompt recognition, structured maneuvers, and coordinated teamwork greatly improve outcomes for both mother and baby.
Click here to contact us with any questions.
Maternal 911 Education Systems, LLC is a leader in emergency obstetrics and team training, improving outcomes through education and evidence-based practice. Maternal 911 Education Systems, LLC is led by a team of experts in emergency obstetrics and maternal safety, dedicated to improving outcomes through evidence-based, team-centered education. Passionate about maternal health education, Maternal 911 advocates for evidence-based practices and interdisciplinary team training. Their mission is to reduce pregnancy risks through education and emergency training. Learn more at maternal911.com.
Disclaimer: Educational use only — not a substitute for clinical judgment or local protocols.
Sources:
Hill DA, Lense J, Roepcke F. Shoulder dystocia: managing an obstetric emergency. Am Fam Physician. 2020;102(2):84-90.
American College of Obstetricians and Gynecologists. Executive summary: neonatal brachial plexus palsy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Neonatal Brachial Plexus Palsy. Obstet Gynecol. 2014;123(4):903-907. doi:10.1097/01.AOG.0000445583.99408.c0
Gurewitsch Allen E. Prescriptive and proscriptive lessons for managing shoulder dystocia: a technical and videographical tutorial. Am J Obstet Gynecol. 2024;230(2):115-125. doi:10.1016/j.ajog.2023.10.014
Lau SL, Sin WTA, Wong L, et al. A critical evaluation of the external and internal maneuvers for resolution of shoulder dystocia. Am J Obstet Gynecol. 2024;230(3):381-389. doi:10.1016/j.ajog.2023.11.008
Stitely ML, Gherman RB. Shoulder dystocia: management and documentation. Semin Perinatol. 2014;38(4):214-220. doi:10.1053/j.semperi.2014.04.002







